
By Leanne Berry
The incredible capacity of humans and other animals to process and experience physical sensations is largely thanks to an intricate web of sensory neurons that extend throughout our bodies. These neurons transduce electrical signals leading to conscious perception of the physical sensation. However, during medical procedures, sensory neurons can lead us to experience intense and unrelenting pain, which can cause our bodies to go into shock. This is where anaesthesia comes in. Anaesthetics enable medical procedures on patients to be conducted in a more comfortable manner by blocking the transmission of pain signals through the nervous system.

Hippocrates referred to anaesthesiology in his writings at approximately 400 BCE. However, it was another two millennia before a mechanism and process were devised for anaesthesia to be safely administered. In 1846, Dr. William Morton performed surgery by “etherisation” of the patient. In 1847, Dr. James Simpson popularised the use of chloroform as an anesthetic. Modern anaesthetic drugs can now be administered in a variety of ways, through gas inhalation, intravenously or by injection into a region of the body.
There are three primary branches of anaesthesia; general anaesthesia, local anaesthesia and regional anaesthesia. General anaesthesia is a drug-induced reversible state consisting of unconsciousness, immobility, amnesia and with maintenance of homeostasis. General anaesthetics generally act on the receptors on the post-synaptic neuron. The activation of the receptors leads to a change in permeability of the membrane to specific ions. This results in a change in membrane potential which excites or inhibits the succeeding neuron depending on the particular state of the synapse in question.
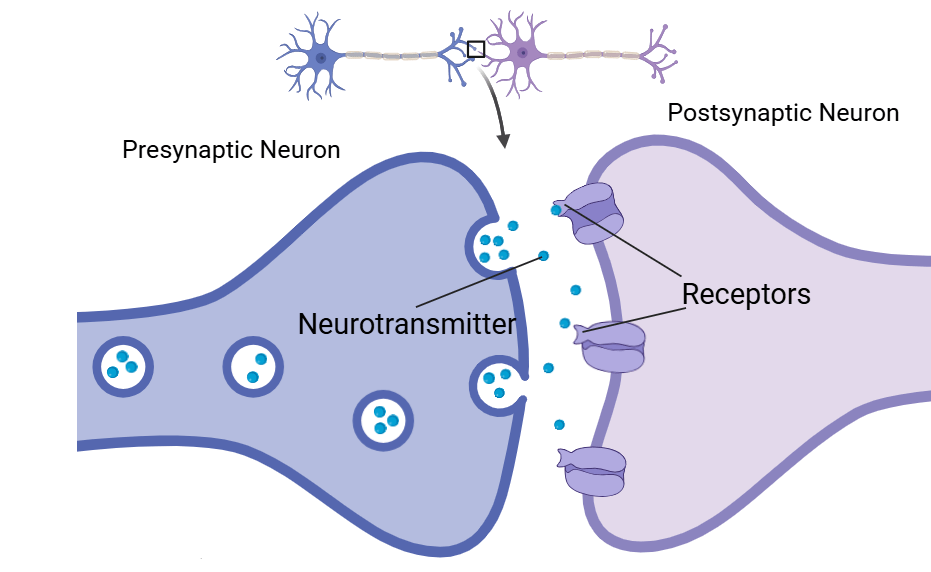
Propofol is one the most commonly used intravenously administered anesthetic agents in general anesthesia practices. Propofol directly interacts with the neurotransmitter gamma-aminobutyric acid (GABA), the brain’s main inhibitory neurotransmitter, to activate the GABA-A receptor on the post-synaptic neuron in the central nervous system (CNS). GABA-A receptors are ligand-gated selective chloride ion channels. This interaction promotes the inhibitory function of GABA. The binding of propofol to the GABA-A receptor results in an influx of chloride ions through chloride ion channels, resulting in sustained hyperpolarisation of the resting cell membrane potential. The most important structural feature of propofol for binding to the GABA-A receptor is the proton of the hydroxyl group on the aromatic ring. The hydroxyl group has a high affinity for hydrogen bonding to an acceptor
group on the GABA-A receptor. Once propofol distributes across the plasma membrane, skeletal or adipose tissue, the drug is readily metabolised into inactive water soluble metabolites.
Conversely, local anaesthetics are most commonly administered topically, by infiltrative anaesthesia or by peripheral nerve blocks. Regional anaesthetic procedures include an epidural anaesthetic, which is administered via needle between vertebrae into epidural space to temporarily block pain from the waist down.
Lidocaine is a widely used local anaesthetic agent. It contains an aromatic ring, a structure that allows the drug to permeate through the lipophilic cellular membrane. The hydrophilic amino group contributes to the molecule’s solubility in water. Unlike propofol, lidocaine applies its anaesthetic mechanism on the peripheral nervous system (PNS) as well as the CNS by diffusing through the lipophilic cellular membrane and binding to the voltage-gated sodium channel from the intracellular side.The reversible binding of the lidocaine to the presynaptic neuron inhibits the influx of sodium ions through the channel. This prevents the propagation of an action potential along the nerve. Lidocaine is initially metabolised in the liver where the alkyl groups are removed from the amine. The amide is then more readily hydrolysed to produce the desired metabolites.
Ropivacaine is a more modern anaesthetic. It features a greater anaesthetic potency due to its higher lipid solubility, longer acting properties but higher cardiotoxicity than lidocaine. Ropivacaine can selectively block nerve fibres that are responsible for pain transmission and not interfere with nerves that dictate motor function.Ropivacaine is extensively metabolised in the liver in a similar manner to lidocaine using cytochrome P450 enzymes.
Anaesthesia has progressed significantly since its introduction 180 years ago, enabling safer,
pain-free surgical practice, faster recovery and better overall clinical outcomes.


Leave a comment