
By Keeva O’Reilly
Haemochromatosis is known as the Celtic disease or the ‘Celtic Curse’, since it affects so many Irish people. This is an inherited condition which causes excessive amounts of iron to be absorbed from the diet and stored in the body. If left untreated, the high levels of iron cause damage to the pancreas, liver, heart and other organs. Overtime, these high levels of iron could contribute to diabetes, heart disease and cirrhosis.
Though there is no cure for haemochromatosis, the traditional way of managing it was through phlebotomy or frequent blood donation. The downside to donating blood in Ireland are all the criteria that the individual must meet before being able to do so. For example, as stated by the Irish Blood Transfusion Service, people who suffer from anemia, are underweight or who have HIV are not allowed to donate blood. The eligibility list is so strict that even individuals who were unlucky enough to have ever been bitten by a monkey can never give blood. Thanks to chelation therapy, people who do not meet the stringent requirements can keep their iron levels under control.
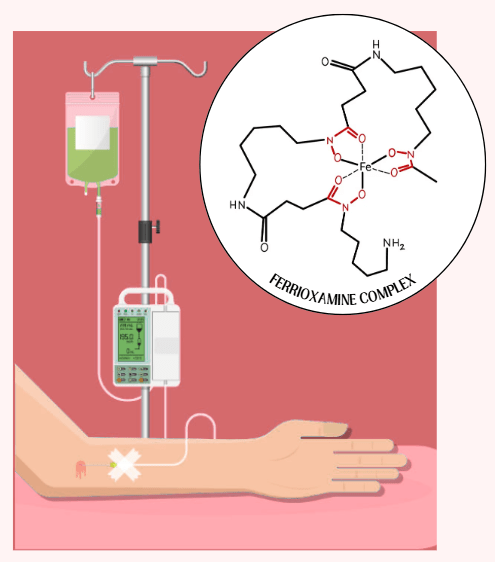
Chelation therapy became mainstream around the 80s when the drug, deferoxamine became more widely available. Deferoxamine is a highly selective chelating drug. When administered into the body, it binds to the free Fe3+ ions to form a stable ferrioxamine complex, while leaving the body’s essential iron untouched. Only the iron that would otherwise cause organ damage binds to the drug, meaning the transport of oxygen through the bloodstream via haemoglobin is unaffected. The ferrioxamine complex (and the excess iron) is then removed from the body as urine.
Deferoxamine is typically administered via subcutaneous infusion overnight, but this must be readily monitored. As chelation therapy continues to advance, the methods of treatment continue to become less invasive. For example, the chelating drugs deferasirox and deferiprone can be taken orally. These advances significantly increase the quality of life for those suffering from haemochromatosis.
The downside to chelation therapy in haemochromatosis treatment is that it is not a cure. Sufferers will have to continue either chelation therapy or phlebotomy for the rest of their lives in order to keep their symptoms at bay. Chelation therapy takes longer to work than phlebotomy, nevertheless it is more accessible to those who suffer from chronic illness or other issues where blood donation would not be possible. Chelation therapy is also very costly and often not covered by insurance.
The discovery of chelation therapy did not have its roots in managing haemochromatosis. It was discovered by British scientists during World War II as a way of combating arsenic poisoning. The first chelating agent used was an organic compound called dimercaprol, acting as an antidote for lewisite poisoning. Later, in the 1950s, a compound called ethylenediaminetetraacetic acid (EDTA) was administered to American factory workers to remedy lead poisoning. It was found that chelating agents could be used to remove a wide range of heavy metals from the body and is still an area that scientists are continuing to work on.
In conclusion, chelation therapy helps to make the ‘Celtic Curse’ a lot more manageable. It provides an alternative to phlebotomy, which allows more people to have access to the treatment they need. With continued research, scientists will develop less invasive and lower cost methods for administering chelation drugs.

Leave a comment